
4/2006

by John Eberhard, FAIA
Good design can speed patient recovery and help visitors find their way.
Have you ever had a feeling of panic when you cannot find your way? If someone you really care about is a patient in a hospital and you get lost finding his or her room, you know about this frustration.
 But imagine you are a 70-year-old person going to visit your critically
ill spouse. The helpful receptionist at the front desk told you what
room to go to and perhaps some general information about how to get there.
Eventually you get hopelessly lost in the endless corridors of the hospital,
however, and you break down in tears of anxiety. You would be having
an experience that is all too common—you are being stressed because
of difficulty in “wayfinding.” This concept of finding one’s
way from one place to another is becoming a major concern of neuroscience
research, as discussed below.
But imagine you are a 70-year-old person going to visit your critically
ill spouse. The helpful receptionist at the front desk told you what
room to go to and perhaps some general information about how to get there.
Eventually you get hopelessly lost in the endless corridors of the hospital,
however, and you break down in tears of anxiety. You would be having
an experience that is all too common—you are being stressed because
of difficulty in “wayfinding.” This concept of finding one’s
way from one place to another is becoming a major concern of neuroscience
research, as discussed below.
Stress is a product of the brain
Dr. Esther Sternberg, a member of the Board of the Academy of Neuroscience
for Architecture, says that researchers are now making advances showing
the actual pathways connecting the areas of our brain that control
immunity with those that generate feelings and thoughts. In The
Balance Within: The Science Connecting Health and Emotions (W.H. Freeman and
Company) Dr. Sternberg explains the connecting mechanisms and their
significance—how nerves, molecules, and hormones connect the
brain and immune system; how the immune system signals the brain and
affects our emotions; and how our brain can signal the immune system,
making us more vulnerable to illnesses. Neuroscientists have not only
discovered the links, but have demonstrated how they work and what
the implications can be for treatable and chronic diseases. What you've
known intuitively (that being exhausted or stressed can make you more
vulnerable to illness) is now understood scientifically.
Neurotransmitters
Our abilities to see, hear, remember, and fear danger and desire happiness
all involve synaptic transmission of chemical signals between the neurons
in our brain. What makes it possible for the brain to distinguish between
a sound or a sight, a memory or a perception, a fear or a desire is
the interaction between receptors in specific areas of the brain and
the chemical signals carried by neurotransmitters.
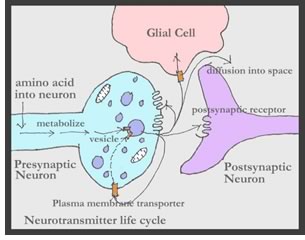
If you have read the previous neuroscience articles in AIArchitect, you will remember that synapses are the gaps between neurons across which information is transmitted. Most synapses rely on a chemical transmitter, called a neurotransmitter, to carry information from one neuron to other neurons. They carry a message from the presynaptic neuron to the postsynaptic neuron in the form of a chemical code created by their molecular structure. Once the neurotransmitters are released into the synaptic space, they look for receptors that will fit their code. This is something like a lock and key, where only certain keys will fit certain locks.
When a neurotransmitter is first produced inside the presynaptic neuron, it goes through chemical changes by which energy is provided for vital activities and new material is assimilated (in other words, it has been “metabolized”). It is then stored in a vesicle, which is a small sack, in which it is kept from degradation until it is ready to be released, like keeping fruit in a container in the refrigerator until it is ready to be eaten. Once it is released into the synaptic space, it is ready to be acquired by receptors in the postsynaptic neuron. (You did not really need to know all of this detail, but I thought it would be useful to know that there are amazingly complicated things happening even at this level of the brain. And, most importantly, even though our brains are essentially all alike it is the subtle differences in how these processes produce minor changes in the networks of the brain that makes each of us unique.)
 You might wonder why the brain was not designed to simply use electrical—instead
of chemical—connections between neurons. The answer appears to
be the enormous difference in how potent a chemical connection can be.
In an electrical connection, only a small difference in the electrical
charge can be transmitted. By contrast, in a chemical transmission, a
single action potential in a small presynaptic terminal can generate
a postsynaptic potential as large as tens of millions of millivolts.
You might wonder why the brain was not designed to simply use electrical—instead
of chemical—connections between neurons. The answer appears to
be the enormous difference in how potent a chemical connection can be.
In an electrical connection, only a small difference in the electrical
charge can be transmitted. By contrast, in a chemical transmission, a
single action potential in a small presynaptic terminal can generate
a postsynaptic potential as large as tens of millions of millivolts.
Different types of neurotransmitters
There are many “classical” neurotransmitters as well as dozens
of neuropeptides (specialized molecules) that function as transmitters.
The simple explanation for why there are so many types is that a neuron
needs to distinguish between the multiple inputs that bring information
to it.
The “most important” neurotransmitters
- Glutamate is the main transmitter for the brain because it can fulfill both speed and excitation roles. It is a key ingredient in forging the links between neurons that are the basis of learning and forming long-term memories.
- GABA is released by inhibitor neurons. It acts as a guard against excessive input from glutamate transmitters. Without GABA inhibition, neurons would send out action potentials continuously under the influence of glutamate, and would eventually fire themselves to death.
- Dopamine controls arousal levels in many parts of the brain and is vital for giving physical motivation.
- Serotonin is sometimes called the “feel-good” chemical because high levels of it are associated with serenity and optimism. It has a profound effect on mood and anxiety. But it also affects many other areas, including sleep, pain, appetite, and blood pressure.
- Acetylcholine controls activities of the brain associated with attention, learning, and memory. People with Alzheimer’s disease usually have low levels of acetylcholine in their cerebral cortex.
Building intellectual bridges between neuroscience and architecture
Neuroscience concepts, such as neurotransmitters and their message system
within the brain, have been included in a series of workshops the Academy
of Neuroscience for Architecture (ANFA) has organized over the past
three years. (Go to the ANFA Web site, www.ANFArch.org, select “Activities,” and
then select “Publications” to read about these workshops.)
By bringing together 15 architects and 15 neuroscientists for a day
or two of serious interaction, we have explored a number of building
types. Health-care facilities have been the focus of three of these
workshops, held at the conference center of the National Academy of
Science in Woods Hole, Mass. This gracious meeting place, located directly
on the water surrounding the NAS property, is extremely conducive to
stimulating productive discussions between our two quite different
disciplines.
A large number of hypotheses have been produced as the outcome of these interactions between architects and neuroscientists. Some of the hypotheses are general statements that the group judged to be intuitively correct—but still open to verification. Others are clear, intellectual statements that could serve as a basis for PhD and post-doctoral experiments in neuroscience laboratories.
 When a scientist describes a hypothesis, he or she would hope to provide
convincing evidence (by conducting a series of tests) that the hypothesis
(or the concept underlying it) is correct. After a series of tests have
been done, all of which seem to support the original hypothesis (or,
to put it another way, give no evidence that the hypothesis is false)
it is considered reasonable to treat the hypothesis as true. There is
always the possibility that later research will produce results contrary
to the initial findings, but if reviews of the initial tests all seem
to support the hypothesis, then the statement can be used as “evidence.” Consequently,
if any of the following hypotheses were to succeed in passing these critical
tests and the subsequent reviews, then architects would be in a position
to use the results as evidence for their design decisions.
When a scientist describes a hypothesis, he or she would hope to provide
convincing evidence (by conducting a series of tests) that the hypothesis
(or the concept underlying it) is correct. After a series of tests have
been done, all of which seem to support the original hypothesis (or,
to put it another way, give no evidence that the hypothesis is false)
it is considered reasonable to treat the hypothesis as true. There is
always the possibility that later research will produce results contrary
to the initial findings, but if reviews of the initial tests all seem
to support the hypothesis, then the statement can be used as “evidence.” Consequently,
if any of the following hypotheses were to succeed in passing these critical
tests and the subsequent reviews, then architects would be in a position
to use the results as evidence for their design decisions.
1. Hypothesis on windows in patient rooms: Windows influence the healing process because variations in the perceived environment affect brain processes that in turn alter outcome measures associated with positive patient experiences.
The following report by Dr. Roger Ulrich became the premise on which this hypothesis was based:
“Between 1972 and 1981 in a Pennsylvania hospital, 23 pairs of patients, all undergoing cholecystectomy [gall bladder removal] operations, were selected by matching sex, age (within five years), being a smoker or a non-smoker, obese or within normal weight limits, general nature of previous hospitalization, year of surgery (within six years), and floor level. One of each pair was assigned to a room with a view of a brick wall (like the view on the right), whilst the other had a view of a ‘natural scene’ with deciduous trees (like the view on the left). Patients with a natural view spent a shorter time in the hospital than those with the brick wall view (7.96 days compared with 8.70 days per patient) and had fewer negative notes made about them (1.13 per patient compared with 3.96 per patient). The ‘natural view’ group requested significantly fewer doses of analgesics in the period between two and five days after surgery, when patients are most in control of their own pain relief. These results indicate that patients with a ‘natural view’ make a recovery, with less pain relief needed.” Ulrich, R.S., “View Through a Window May Influence Recovery from Surgery,” Science magazine, v.224, 1984, pp. 420-42.1.
 Although the research by Ulrich has provided a strong “indication” for
the value of rooms with a view of nature, the above hypothesis would
potentially provide evidence of why this is true.
Although the research by Ulrich has provided a strong “indication” for
the value of rooms with a view of nature, the above hypothesis would
potentially provide evidence of why this is true.
2. Hypothesis on the value of privacy for patients: Privacy mechanisms in humans are strongly related to the neurological mechanisms inherent in our species with respect to questions of personal safety, territoriality (i.e, “this is my space”), eating of food, using the bathroom, and eavesdropping.
There is a related issue of privacy with respect to patient/doctor discussions that is a concern of the attending physicians. There are also related design decisions about the acoustic and lighting environment and the control by patients of unwanted noise or lights. The concern with patients being able to exert control of these variables is easily determined by observation. What we would want to explore with neuroscience methods is how the sense of privacy is resident in the brain and what variables in the architectural setting are shown to trigger related anxieties. From what you have been learning about the brain, you will understand that the part of the brain called the amygdala is likely to be involved, since it is the “seat of fears and phobias.”
3., 4. Two hypotheses on “wayfinding” experiences: There are certain kinds of landmarks (or place markers) that are more easily associated with path recognition by the brain.
There is a measurable difference in the brains of people who might be called “wayfinding gifted” as contrasted to those who are “wayfinding challenged.”
While the term “wayfinding” is not one used by most people, its meaning seems clear: it defines how one finds the way from one location to another. Thus, people visiting a hospital (as indicated in the opening paragraph) can become easily distressed when they get lost trying to find a specific room. The first hypothesis is obviously not limited to hospitals. Children in a large school building, workers in complicated office buildings, drivers in areas of a city being visited for the first time (and often even after several visits) all have a need to find their way. It seems likely from what we have been discussing in these articles (see January article) that the hippocampus is very much involved in wayfinding.
Experiments made with rodents placed in tanks of milky liquid and given a platform they can swim to because they want to escape the challenge of swimming, soon learn the specific location of the platform. They will swim to the area where the platform was located even when it is removed. Research has clearly shown that the C1 area of the hippocampus is where these paths are stored once they are experienced. Each time the same trip is made, the record is reinforced until the path can be called “learned.”
5. Hypothesis on providing calming environments for Alzheimer’s residents: There are genetically coded memories associated with the concept of a hearth by a fireplace or a garden that are still accessible to those with Alzheimer’s disease. These memories, when reinforced by design features of a residential Alzheimer’s unit, contribute to a sense of calm in the minds of the residents.
While there is a good deal of empirical evidence that design features such as a fireplace with a hearth and/or a garden are much enjoyed by residents of Alzheimer’s facilities, there is no neurological evidence to answer the question of why this would be true. You may remember a discussion in an earlier article (see February article) about “explicit” and “implicit” memories. Even though patients with Alzheimer’s disease lose the ability to recall explicit memories (someone they should recognize, or what day of the month it is), they still have other parts of their brains that are responding in a non-conscious way to implicit memories, including those that were laid down by genes from their DNA.
Providing art for calming patients
Henry Domke, MD, who is a physician as well as a photographer, produces
lovely photographs to be used in health-care facilities as “calming” elements
in architectural settings. The photograph on the wall in the illustration
below is called “Big Bluestem” after the native warm-season
grass he used as his subject. He tells me, “The picture shows
the grass in full flower. I photographed this on the prairie where
I live, the Prairie Garden Trust. All of my images are photographed
in the wild and they are all native (never garden) flowers and animals.” (For
more information, visit Dr. Domke’s Web page.)
 Dr. Domke has well-developed—but intuitive—knowledge of
how to photograph plants and animals that will produce images clearly
shown to contribute to a calming environment. One day, neuroscientists
may learn how the brain produces this response.
Dr. Domke has well-developed—but intuitive—knowledge of
how to photograph plants and animals that will produce images clearly
shown to contribute to a calming environment. One day, neuroscientists
may learn how the brain produces this response.
What can architects learn from this?
Nancy Andreasen, PhD, has been studying how our brains contribute to
our creativity. For example, how would we benefit in being able to
design better hospitals? She asks: “How do human beings actually
create the novel, beautiful, and useful ideas, images, and other products
that are the hallmark of creativity?” She answers: “Deceptively
simple as thus stated, this is in fact a very complex question. Philosophers,
psychologists, and psychiatrists have been preoccupied with exploring
answers to this question for many years. Ultimately, neuroscience will
provide new answers, showing how the creative products arise from a
process that occurs in an individual brain.” (From The
Creating Brain: the Neuroscience of Genius, Dana Press, 2005.)
In the first four AIArchitect articles, we have explored together concepts emerging from research by neuroscientists. Today, we looked at how some of these concepts can be linked to hypotheses about design criteria for health-care facilities. In the next few articles, we will be exploring additional hypotheses related to K-6 classroom design, experiences in sacred places, what we are learning about the design of facilities for our aging population, and experiences in retail and entertainment facilities. I hope you will join us in exploration of the potential of these exciting new developments.
Copyright 2006 The American Institute of Architects.
All rights reserved. Home Page ![]()
![]()
For more information, visit the Academy of Neuroscience for Architecture Web site.
Drawings by the author.
Read the other four articles in this series:
• See the Space and Hear the Sound of Music
How we use the brain and mind to see and hear ![]()
• Thanks for the Memories
The brain, the mind, and creation of memories ![]()
• You Need to Know What You Don't Know ![]()
• How We Use the Brain and Mind to Smell, Taste, and Touch ![]()
Read this introductory article by the author:
The Neuroscience in A
Christmas Carol
A tale of conception, perception, and proprioception ![]()
![]()
![]()
![]()