| A Patient Room Prototype: Bridging Design and Research
Summary: Patients, their families, and caregivers alike spend a significant amount of time in hospital inpatient rooms. Despite the number of hours these rooms are occupied, and the number of variations of room designs in hospitals, there has not been a comprehensive effort to study the performance of new room concepts. To bridge that knowledge gap, Dina Battisto, PhD, MArch, and David Allison, AIA present their Patient Room Prototype in the latest edition of the AIA Academy Journal of the Academy of Architecture for Health.
 The authors focused their research using an interdisciplinary and
participatory design process involving designers, researchers, product
manufacturers, clinicians, and administrators from both academia
and practice. Their overarching goal is to integrate design and research
more precisely to develop new, speculative patient care environments.
A premise guiding the process is that user-centered patient-room
concepts will ultimately improve usability outcomes, including efficiency,
effectiveness, safety, and satisfaction for patients, families, and
staff. The authors focused their research using an interdisciplinary and
participatory design process involving designers, researchers, product
manufacturers, clinicians, and administrators from both academia
and practice. Their overarching goal is to integrate design and research
more precisely to develop new, speculative patient care environments.
A premise guiding the process is that user-centered patient-room
concepts will ultimately improve usability outcomes, including efficiency,
effectiveness, safety, and satisfaction for patients, families, and
staff.
Problems
Studies to date suggest that conditions in patient room environments can positively or negatively impact stress, staff injuries, patient safety, operational efficiency, staff satisfaction, nursing turnover, and medical errors. These issues may result from many factors, including inadequate lighting, absence of daylighting, noise, double occupancy rather than single occupancy rooms, lack of standardized rooms, materials, and layout. Additional studies show unit physical layout and interiors of the work environment affect nurse workload.
To explore the integration of design and research related to new design concepts, the authors present a project for a hospital Patient Room Prototype (PRP). The PRP is a concept that employs an iterative design-research process informed by both first-hand (practical) knowledge and second-hand (theoretical) knowledge. Further, it engages in an interdisciplinary participatory process infused with periodic informal and formal systematic evaluations aimed at advancing each design-research input and feedback cycle.
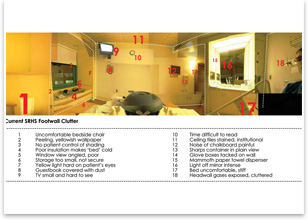
 The extended stay of multiple observers in a variety of room configurations
yielded many astute and detailed observations that might otherwise
be overlooked in a casual walkthrough. Poor finish and millwork details,
the wear and tear of finishes and features, the inability to clean
surfaces and in corners adequately, and the lack of functionality
of certain features become particularly noticeable when encountered
over an extended period of time. A significant condition evident
in all observations was the overwhelming amount of visual noise or
institutional clutter in constant view of the patient and family. The extended stay of multiple observers in a variety of room configurations
yielded many astute and detailed observations that might otherwise
be overlooked in a casual walkthrough. Poor finish and millwork details,
the wear and tear of finishes and features, the inability to clean
surfaces and in corners adequately, and the lack of functionality
of certain features become particularly noticeable when encountered
over an extended period of time. A significant condition evident
in all observations was the overwhelming amount of visual noise or
institutional clutter in constant view of the patient and family.
Solutions
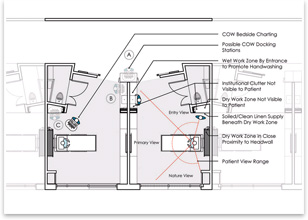
In contrast, the authors looked at a layout that features orientation of the single-occupant rooms so that the foot wall (the wall the patient faces) is clear of clinical equipment and has an adequately sized television screen and clock. Additionally, the clinical equipment is placed at the head wall so the patient is not constantly reminded that he or she is in a hospital environment. The views to the hallway are open and clear so that the patient knows who is coming in, and sight lines to the outside allow a sense of connection to comforting views of the rest of the world. The positioning of wet and dry work areas encourages hospital staff to practice routine hygiene and medical procedures efficiently. Bedside record-keeping equipment further maximizes timeliness and accuracy.
To read this article in its entirety, as well as other peer-reviewed articles on hospital facility design to accommodate obese patients, using simulation in health-care facility design, and “Reinventing the Academic Medical Center,” visit the AIA Academy Journal page on AIA.org.
Excerpted from the AIA Academy Journal, the online journal of peer-reviewed articles published by the AIA Academy of Architecture for Health.
|